Most often, this test is done to measure the strength of your immune system if you have been diagnosed with human immunodeficiency virus (HIV) infection and to monitor treatment; occasionally, it may be used with other conditions (see Common Questions below).
CD4 Count
CD4 Count
Also Known As
T4 Count
T-helper Cells
Formal Name
CD4 Lymphocyte Count; CD4 Percent
This article was last reviewed
on
This article waslast modified
on December 4, 2017.
At a Glance
Why Get Tested?
When To Get Tested?
When you are first diagnosed with HIV infection to get a baseline assessment of your immune system; about every 3 to 6 months after starting antiretroviral therapy (ART) to check whether you are responding to treatment; if you have responded well to treatment, you may then be tested every 6 to 12 months.
Sample Required?
A blood sample drawn from a vein in your arm
Test Preparation Needed?
None
Accordion Title
Common Questions
-
How is it used?
CD4 counts are most often used, along with an HIV viral load, to evaluate the immune system of a person diagnosed with human immunodeficiency virus (HIV) infection and to monitor effectiveness of antiretroviral treatment (ART or ARV), also called highly active antiretroviral therapy (HAART).
CD4 cells are types of white blood cells called T lymphocytes or T cells that fight infection and play an important role in immune system function. They are made in the thymus gland and they circulate throughout the body in the blood. (See the "What is being tested?" section for more details.)
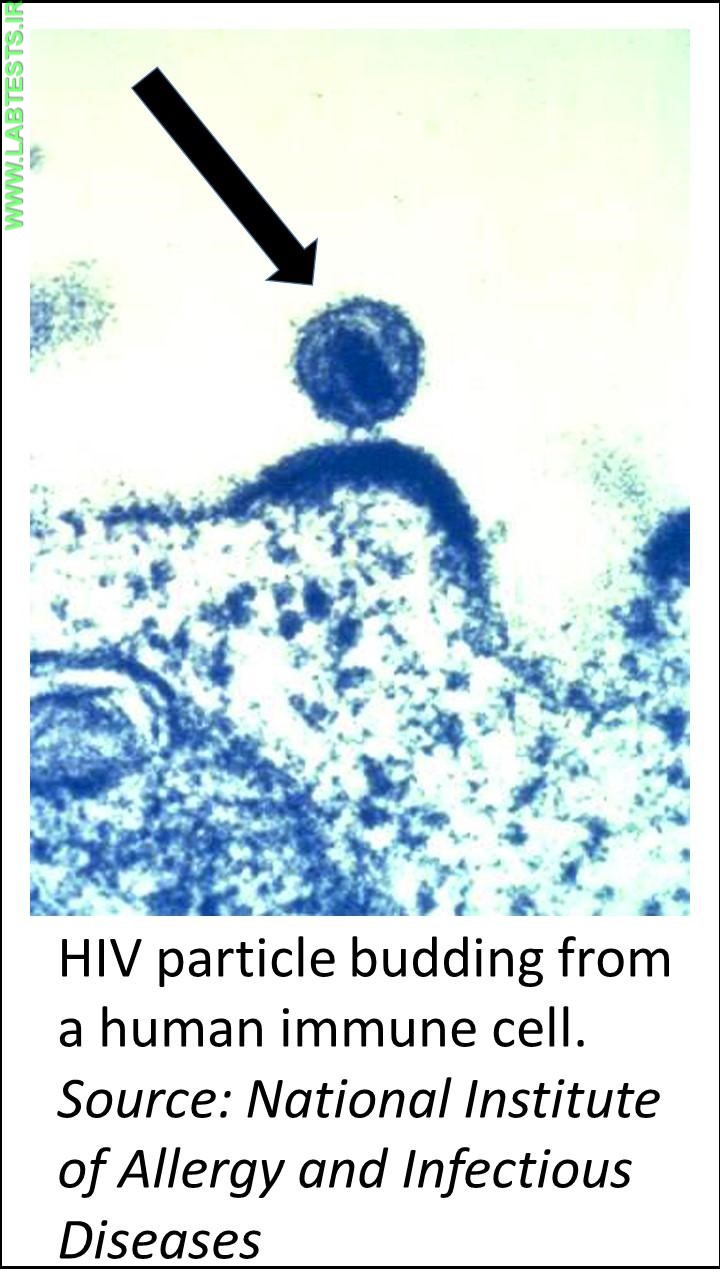
CD4 cells are the main target of HIV. The virus enters the cells and uses them to make copies of itself (replicate) and spread throughout the body. HIV kills CD4 cells, so if an HIV infection is not treated, the number of CD4 cells will decrease as HIV infection progresses.
It is recommended that all individuals diagnosed with HIV infection receive antiretroviral treatment as soon as possible, including pregnant women, to reduce the risk of disease progression. People typically take at least three drugs from two different classes in order to prevent or minimize virus replication and the emergence of drug-resistant strains. Combinations of three or more antiretroviral drugs are referred to as highly active antiretroviral therapy or HAART.
Since CD4 cells are usually destroyed more rapidly than other types of lymphocytes and because absolute counts can vary from day to day, it is sometimes useful to look at the number of CD4 cells compared to the total lymphocyte count. The result is expressed as a percentage, i.e., CD4 percent.
The results can tell a health practitioner how strong a person's immune system is and can help predict the risk of complications and debilitating opportunistic infections. CD4 counts are most useful when they are compared with results obtained from earlier tests. They are used in combination with the HIV viral load test, which measures the amount of HIV in the blood, to monitor how effective ART is in suppressing the virus and determine the risk of progression of HIV disease.
Sometimes, CD4 tests may be used along with a test for CD8 cells to help diagnose or monitor other conditions such as lymphoma, organ transplantation, and DiGeorge syndrome (see Common Questions #4). CD8 cells are another type of lymphocyte that identify and kill cells that have been infected with viruses or that have been affected by cancer.
-
When is it ordered?
A CD4 count is usually ordered along with an HIV viral load when a person is first diagnosed with HIV infection as part of a baseline measurement. After the baseline, a CD4 count will usually be ordered at intervals over time, depending on a few different factors.
The following table summarizes recommendations* for the timing of CD4 counts and viral load testing:
Clinical Status of Patient Viral Load CD4 Count When first diagnosed Test performed Test performed After initiating ART Within 2-4 weeks and then every 4-8 weeks until virus is suppressed (undetectable) 3 months later During the first 2 years of stable ART Every 3-4 months Every 3-6 months After 2 years of stable ART, virus undetectable, and CD4 greater than 300 cells/mm3 Can extend to every 6 months Annually; if CD4 consistently greater than 500 cells/mm3, monitoring is optional After changing ART due to side effects or simplifying drug regimen in a person with suppressed virus After 4-8 weeks, to confirm drug effectiveness Monitor according to prior CD4 count and the amount of time person has been on ART, as detailed above After changing ART due to increased viral load (treatment failure) Within 2-4 weeks and then every 4-8 weeks until virus undetectable Every 3-6 months While on ART and viral load is consistently greater than 200 copies/mL Every 3 months Every 3-6 months With new HIV symptoms or start of new treatment with interferon, corticosteroids or cancer drugs Every 3 months Perform test and monitor according to health status (e.g., new HIV symptoms, opportunistic infections) *Adapted from Guidelines for the Use of Antiretroviral Agents in HIV-1–Infected Adults and Adolescents, Table 4. Recommendations on the Indications and Frequency of Viral Load and CD4 Count Monitoring.
-
What does the test result mean?
A CD4 count is typically reported as an absolute level or count of cells (expressed as cells per cubic millimeter of blood). A normal CD4 count ranges from 500–1,200 cells/mm3 in adults and teens. Sometimes results are expressed as a percent of total lymphocytes (CD4 percent).
In general, a normal CD4 count means that the person's immune system is not yet affected by HIV infection. A low CD4 count indicates that the person's immune system has been affected by HIV and/or the disease is progressing. However, any single CD4 test result may differ from the last one even though the person's health status has not changed. Usually, a health practitioner will take several CD4 test results into account rather than a single value and will evaluate the pattern of CD4 counts over time.
CD4 counts that rise and/or stabilize over time may indicate that the person is responding to treatment. If someone's CD4 count declines over several months, a health practitioner may recommend starting prophylactic treatment for opportunistic infections such as Pneumocystis carinii (jiroveci) pneumonia (PCP) or candidiasis (thrush).
-
Is there anything else I should know?
The CD4 count tends to be lower in the morning and higher in the evening. Acute illnesses, such as pneumonia, influenza, or herpes simplex virus infection, can cause the CD4 count to decline temporarily. Cancer chemotherapy can dramatically lower the CD4 count.
The CD4 count does not always reflect how someone with HIV disease feels and functions. For example, some people with higher counts are ill and have frequent complications, and some people with lower CD4 counts have few medical complications and function well.
The Centers for Disease Control and Prevention (CDC) considers people who have an HIV infection and CD4 counts below 200 cells/mm3 to have AIDS (stage III HIV infection), regardless of whether they have any signs or symptoms.
-
How is HIV infection diagnosed?
HIV infection is usually screened for with an HIV antibody test or a combination test for HIV antibody and antigen (p24). If the screening test is positive, it must be followed with another test, such as a second antibody test that can differentiate HIV-1 and HIV-2. If results of the first and second test do not agree, then the next test to perform is an HIV-1 RNA test (nucleic acid amplification test, NAAT). If either the second antibody test or the HIV-1 RNA is positive, then the person tested is diagnosed with HIV infection. Read the article on HIV Antibody and HIV Antigen (p24) for more details.
-
What are some common opportunistic infections I might get if I have an HIV infection?
Examples include fungal infections such as candidiasis and other infections such as tuberculosis or those caused by nontuberculosis mycobacteria. The Centers for Disease Control and Prevention (CDC) provides a table with examples of common opportunistic infections.
-
What are my treatment options?
You and your healthcare provider should discuss your treatment options to determine what will work best for you. The Mayo Clinic web page HIV/AIDS: Treatments and drugs has detailed information on various therapies.
-
Is a CD4 cell count used in conditions other than HIV infection?
Yes. It may be ordered when a person has had an organ transplant to help evaluate the effect of immunosuppressive medications. In transplantation, the immune system must be suppressed so that it does not attack the transplanted organ and cause rejection. In this case, it is desirable to have low levels of CD4 cells, and a decreased count shows that the drug is working. A CD4 count may be repeated periodically to monitor the effectiveness of therapy.
CD4 counts are sometimes done in conjunction with CD8 counts. CD8 cells are another type of lymphocyte called T-suppressor cell or cytotoxic T cell. CD8 cells identify and kill cells that have been infected with viruses or that have been affected by cancer.
Evaluation of CD4 and CD8 cells may be used to help classify lymphomas. Typically, several markers on the surface of lymphocytes in addition to CD4 and CD8 are evaluated. The tests help determine whether the lymphoma is due to the proliferation of B lymphocytes or T lymphocytes and which specific type. This information is useful in determining appropriate therapy.
These tests may also help diagnose DiGeorge syndrome, a rare congenital disorder characterized by, among other things, low levels of T cells in the blood. For more information on DiGeorge syndrome, visit the Mayo Clinic web site.
-
My report includes a CD4/CD8 ratio. What is it?
It is the number of CD4 cells compared to the number of CD8 cells. In HIV infections, CD4 cells are usually destroyed more rapidly than CD8 cells. Because absolute CD4 counts can vary from day to day, it is sometimes useful to look at the CD4 count compared to the CD8 count to get a clear picture of the health of the immune system. In general, the CD4/CD8 ratio decreases as HIV infection progresses, and the ratio should increase and/or stabilize when treatment is effective.
Related Images

View More